

Study selection
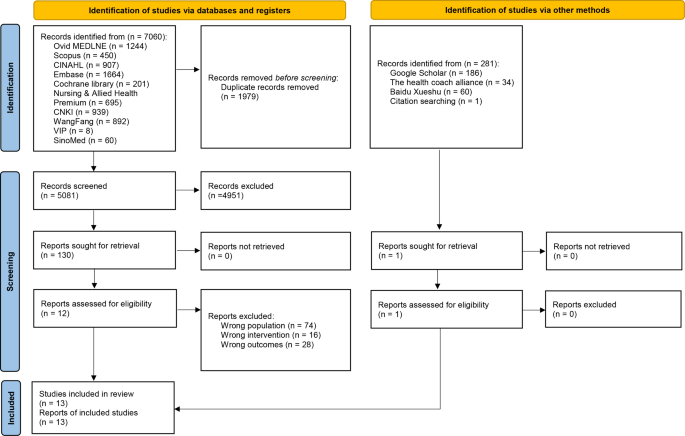
The database search yielded 7,060 records. After removing duplicates, we screened the titles and abstracts of the remaining 5,081 records, resulting in 130 relevant articles for full-text screening. An additional record was identified through citation search, bringing the total to 131 records for full-text review. Of these, 13 studies met the eligibility criteria and were included in our review. The study selection process and results are shown in Fig. 2 [30]. Reasons for the exclusion of studies can be found in Supplementary File 3.
Study characteristics
The studies included in the present review were published between 2009 and 2023. All studies [13, 14, 36, 51,52,53,54,55,56,57,58,59,60] were published in English. The studies were conducted across seven countries, with the majority from the US (n = 4) [13, 52, 54, 60] and Australia (n = 3) [14, 53, 56]. The studies included various types, including qualitative studies (n = 3) [51, 55, 60], case series (n = 3) [36, 52, 57], quasi-experimental studies (n = 2) [56, 59], and mixed-methods studies (n = 5) [13, 14, 53, 57, 58]. The purposes of the studies included assessing the impact of coaching (n = 6) [13, 55, 57,58,59,60], describing participants’ experiences while receiving coaching (n = 2) [36, 51], describing a coaching plan (n = 3) [52,53,54], or exploring the efficacy of coaching (n = 2) [14, 56]. All studies employed self-report measures [61] (e.g., questionnaire, report, in-depth interview) [13, 14, 36, 51,52,53,54, 56,57,58,59,60], with only one study [55] utilizing both self-report and observation methods. Table 1 presents the study characteristics in detail.
A total of 507 coachees and 41 coaches participated in the coaching interventions across the 13 studies. Nine studies [36, 51,52,53,54,55,56,57,58] targeted nurse managers, while four studies [13, 14, 59, 60] recruited nurses, doctors, allied health professionals or public health managers. The coaches were primarily nurses and psychologists. The coachees range in age from 30 to 54 years, but the ages of the coaches were not reported. Five studies [36, 52, 55,56,57] focused on middle management level coaches (such as unit managers), two studies [51, 53] focused on the senior management level coaches (e.g., director), four studies [13, 14, 54, 58] included both middle and senior level coaches, and the remaining two studies [59, 60] did not provide information regarding the level of healthcare managers. Detailed descriptions of the participant characteristics can be found in Table 2.
Risk of bias in the studies
The overall assessment for the three qualitative studies [51, 55, 60] resulted in “No or few limitations,” meaning most items in the tool were answered with “yes” [62]. Insufficient descriptions of the recruitment strategy [51, 60] and data collection methods were the weaknesses of the three studies [55] (see Supplementary File 4, Table S1).
The critical assessment scores for the three case series [36, 52, 54] included in this review ranged from five to eight out of a total score of 10. Quality concerns primarily arose due to the lack of clarity about whether the studies included participants consecutively and comprehensively [36, 52]. Additionally, there were concerns about the inadequate reporting of participants’ “clinical information” (information related to the participant’s management experience, such as the level of positions held and the duration of time spent in management roles) [36, 52] (see Supplementary File 4, Table S2).
The two quasi-experimental studies [56, 59] assessed both with an overall bias rating of “Moderate.” One study showed a moderate risk of confounding bias but a low risk of bias in other areas [56]. The other study had moderate risks of both confounding bias and outcome measurement bias, with low risk of bias in the other areas [59] (see Supplementary File 4, Table S3).
The critical appraisal scores for the five mixed-methods studies [13, 14, 53, 57, 58] ranged from 40 to 60% out of a possible 100%. Concerns were identified in all studies regarding Q3.1 (Are all the participants representative of the target population?) and Q5.5 (Do the different components of the studies adhere to the quality criteria for each tradition of the methods involved?). In all studies except one [53], the confounders were not accounted for in the design and analysis. All studies met criteria 1.1, 1.2, 1.3, 3.5, 5.1, 5.2, 5.3, and 5.4 (see Supplementary File 4, Table S4).
The components of coaching interventions
Aims
Most of the coaching interventions aimed to facilitate the development of leadership skills [13, 14, 36, 53, 55, 57, 58, 60] (n = 8) or behaviours [53, 54, 56] (n = 3). The target groups of the coaching interventions included healthcare managers at the middle management level [36, 52, 55,56,57] (n = 5), senior management level [51, 53] (n = 2), and mixed [13, 14, 54, 58] (n = 4) levels (see Supplementary File 5, Table S1).
Ingredients
In seven studies [13, 14, 36, 53,54,55, 58], materials (e.g., handbooks) were provided to the participants. However, the studies did not specify where these materials could be accessed. We identified three categories of coaching in the included studies: internal (n = 1) [55], external (n = 9) [13, 14, 51,52,53, 56,57,58, 60], and mixed (internal and external) (n = 1) [54]. Two studies [36, 59] did not provide information on the category of coaching used. The coaching interventions reported in 10 studies [13, 14, 52,53,54,55,56,57, 59, 60] included three procedures: a pre-evaluation (baseline evaluation) of the variables (e.g., leadership skills), coaching, and a post-evaluation. Three studies did not involve a pre-evaluation [36, 51, 58]. Two studies [14, 57] had coach-coachee matching procedures, eight studies [14, 36, 51,52,53,54, 57, 60] had orientation procedures, three studies [13, 53, 58] had reminder procedures, and only one study [53] had a follow-up procedure. Eight studies [51, 53,54,55,56,57,58,59] involved support activities such as forums, meetings, discourse, role-playing activities, group interactions, discussions, conversations, roundtables, reports, seminars, and homework. Five studies [13, 14, 36, 52, 60] did not provide any information about support activities (see Supplementary File 5, Table S1).
Mechanism
All included studies reported on the mechanism of coaching. Five studies [13, 52, 54, 55, 60] were based on empirical evidence. Among these, two studies [54, 60] only described the positive impact of the coaching intervention without providing details on the pathway or process by which the intervention worked. Three studies [51, 58, 59] were based on theory, specifically the systems psychodynamic perspective [51], a coaching model [58], and coaching psychology [59]. Five studies [14, 36, 53, 56, 57] were based on both theory and empirical evidence: three studies [14, 53, 56] were based on cognitive-behavioural theory, and two studies were based on the adult learning model [57] and organization theory [36], respectively. Among these five studies [14, 36, 53, 56, 57], one study [56] only mentioned the name of the theory, without any information on the pathway or process by which the intervention worked. Regarding empirical evidence, four studies [14, 36, 53, 57] lacked detailed information on the intervention pathway or process (see Supplementary File 5, Table S2).
Delivery methods
Among the 13 studies included, the duration of coaching interventions was not reported in two studies. For the remaining 11 studies, the intervention durations ranged from two days to seven months, with an average of approximately four months. The coaching delivery modes included in-person meetings, telephone calls, videos, and online methods. The interventions described in the studies were delivered individually or through group coaching. The dose of individual or group coaching varied from 45 min to 4 h, and the frequency of the intervention varied from once a week to once a month for a total of 4 to 32 times during the program. The coaches mainly included psychologists, professional coaches, and nurses. The sizes of the target groups varied from 3 to 111. Three studies [51, 52, 55] implemented the intervention in hospital rooms, and one involved an online intervention [36]. One study [13] did not provide any information on the duration, mode, or level of coaching, and nine studies [13, 14, 53, 54, 56,57,58,59,60] did not report the site of the intervention (see Supplementary File 5, Table S2).
The impact of coaching on leadership development
Both qualitative and quantitative data reported the impact of coaching across various outcomes at manager, organization, and staff levels (categories). Twelve studies assessed the perceived impact of coaching using qualitative data [13, 14, 36, 51,52,53,54,55, 57,58,59,60], identifying 34 codes that were then grouped into 11 themes across the three categories. Eight studies measured the impact of coaching using quantitative data [13, 14, 53, 54, 56,57,58,59], with 26 results extracted and categorized into six classes across the same three levels (see Supplementary File 5, Table S3).
Manager level
The qualitative data showed improvements in the following 15 aspects of leadership among healthcare managers, which were well supported by quantitative data: confidence, resilience, reflection and awareness, role clarity, resonant leadership (a leadership style that focuses on how an individual interacts with others and builds positive relationships) [63], interacting with others, relationships with others, perspective taking, developing others, conflict management, leveraging diversity, team development, feedback process, anxiety, stress, health and well-being, and retention. Qualitative data also identified enhancements in systematic thinking, work/life balance, boundary management, leading by example, dealing with issues, mindset, loneliness, management skills, communication skills, and teamwork skills. However, these findings lacked support from quantitative data (see Supplementary File 5, Table S3). Conversely, the quantitative data indicated improvements in solution-focused thinking and depression, which were not supported by qualitative data.
Organization level
The qualitative findings identified improvement in leadership development among healthcare managers in the following three aspects, all were well supported by quantitative data: retention, vision and strategy, and decision-making and change.
However, the qualitative data also showed there was an enhancement in healthcare quality, which was not supported by the quantitative data (see Supplementary File 5, Table S3).
Staff level
The qualitative data showed that coaching interventions have positive impacts on staff health and well-being, knowledge, and work efficiency; however, the quantitative data did not support the latter two aspects (see Supplementary File 5, Table S3).
Participants’ perceptions of coaching for leadership development
Thirty-nine findings from eight studies [13, 36, 52, 54, 55, 57, 58, 60] were identified as describing participants’ perceptions of coaching for leadership development. These findings formed six categories describing the participants’ perceptions of barriers, facilitators, effective components (the components within coaching interventions that participants perceive as effective or valuable) [64], attitudes, and satisfactory aspects (reflecting participants’ satisfaction with the coaching intervention) as well as their suggestions to improve coaching for leadership development (see Supplementary File 5, Table S4).
Barriers
Three studies [13, 36, 58] identified 10 barriers to the implementation of coaching for leadership development: uncertain impacts, time constraints, indifferent attitudes of staff, a lack of real conflicts, multitasking in multiple sites/departments, a lack of proper training, heavy workload, communication difficulties, challenges of completing coaching, and not understanding the relevance to leadership.
Facilitators
Three studies [36, 58, 60] described 11 facilitators of coaching for leadership development: pride in leadership, responsibility and time allocation, position and role in the organization, positive impact and feedback, management training, leadership skills and democratic approach, good relationship with staff, educational level and experience, desire and gratification related to developing staff, commitment, and push from coaching components.
Effective components
Three studies [36, 52, 54] highlighted two effective components of implementing coaching for leadership development: the coaching relationship and the delivery model and level (face-to-face or one-on-one coaching).
Attitudes
Six studies [13, 36, 52, 54, 57, 60] identified nine attitudes toward the implementation of coaching for leadership development. Three studies [13, 52, 57] described six positive attitudes: welcoming progress evaluations, enjoyment, persistence, future participation, recommending to others, and appreciating coaching relationships. Two studies [36, 54] noted that some of the participants were initially skeptical but eventually found the intervention valuable. One study [36] reported that some participants felt bored at the beginning, while another study [60] found that some participants experienced discomfort when seeking feedback from stakeholders.
Satisfactory aspects
Six studies [36, 52, 54, 55, 57, 58] identified four satisfactory aspects of implementing coaching for leadership development: positive impact, coaching components, outside coaching, and overall satisfaction.
Suggestions
Only one study [36] included suggestions from the participants after they experienced the coaching intervention. Three suggestions were mentioned: expanding the reflection/feedback period, expanding the whole training program, and providing concise reading material.
The summary of the results
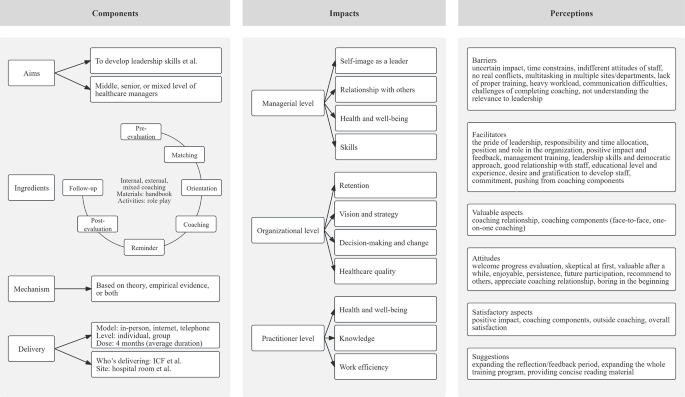
Figure 3 summarizes the results of coaching components, the impact of coaching at manager, organization, and staff levels, and participants’ perceptions of being involved in coaching interventions aimed at developing leadership of healthcare managers.
The summative results of coaching interventions to develop leadership
link
