

Employer-sponsored insurance covers 154 million nonelderly people. To provide a current snapshot of employer-sponsored health benefits, KFF conducts an annual survey of private and non-federal public employers with three or more workers. This is the 26th Employer Health Benefits Survey (EHBS) and reflects employer-sponsored health benefits in 2024.
HEALTH INSURANCE PREMIUMS AND WORKER CONTRIBUTIONS
The average annual premiums for employer-sponsored health insurance in 2024 are $8,951 for single coverage and $25,572 for family coverage. Over the last year, the average single premium increased by 6% and the average family premium increased by 7%. Comparatively, there was an increase of 4.5% in workers’ wages and inflation of 3.2%. Over the last five years, the average premium for family coverage has increased by 24%, compared to a 28% increase in workers’ wages and inflation of 23% [Figure A, Figure B].
The average premiums for small and large firms are comparable for covered workers with single coverage ($9,131 vs. $8,884) and family coverage ($25,167 vs. $25,719). The average premiums for covered workers in high-deductible health plans with a savings option (HDHP/SO) are lower than the overall average premiums for both single coverage ($8,275) and family coverage ($24,196) [Figure C]. On the other hand, average premiums for covered workers enrolled in PPOs are higher than the overall average premiums for both single ($9,383) and family coverage ($26,678). The average premiums for both single and family coverage are lower for covered workers at private for-profit firms and higher for covered workers in private not-for-profit firms. The average premiums for single coverage for covered workers at firms with a larger share of older workers (where at least 35% of the workers are age 50 or older) are higher than the average premium for covered workers at firms with smaller shares of older workers ($9,171 vs. $8,738).
Figure A: Average Annual Worker and Employer Premium Contributions for Family Coverage, 2014, 2019, and 2024
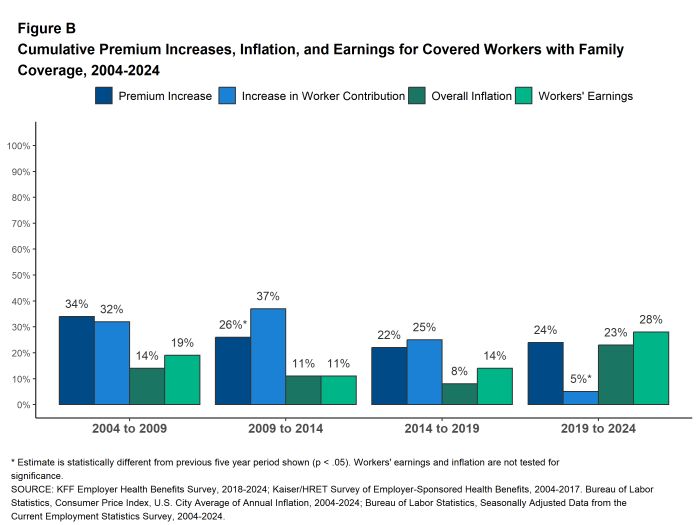
Figure B: Cumulative Premium Increases, Inflation, and Earnings for Covered Workers With Family Coverage, 2004-2024
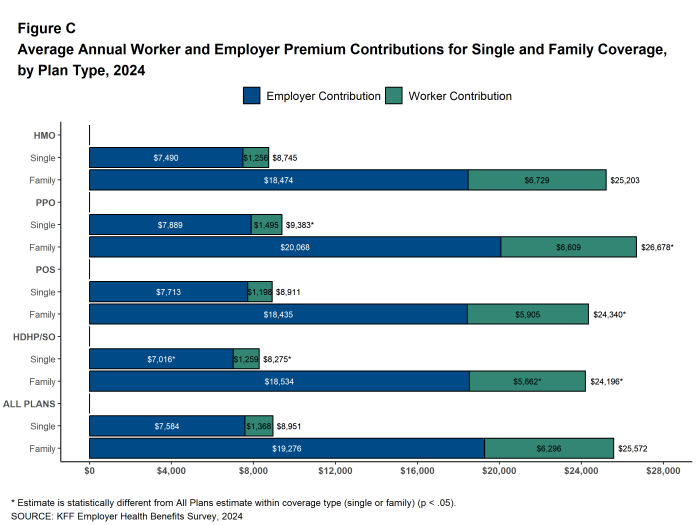
Figure C: Average Annual Worker and Employer Premium Contributions for Single and Family Coverage, by Plan Type, 2024
Most covered workers contribute to the cost of the premium. On average, covered workers contribute 16% of the premium for single coverage and 25% of the premium for family coverage, lower than the percentages contributed in 2023. The average contribution rate for covered workers in small firms is lower than the average contribution rate for covered workers in large firms for single coverage (14% vs.16%) but higher than the average contribution rate for covered workers in large firms for family coverage (33% vs. 23%). On average, covered workers at private, for-profit firms have relatively high premium contribution rates for both single coverage and family coverage.
Thirty-seven percent of covered workers at small firms are enrolled in a plan where the employer pays the entire premium for single coverage. This is the case for only 5% of covered workers at large firms. In contrast, 26% of covered workers at small firms are in a plan where they must contribute more than half of the premium for family coverage, compared to 6% of covered workers at large firms [Figure D].
The average annual dollar amounts contributed by covered workers in 2024 are $1,368 for single coverage and $6,296 for family coverage, similar to the amounts last year. The average contribution amount for covered workers at small firms ($1,204) is lower than the average contribution amount for covered workers at large firms ($1,429). However, the opposite is true for family coverage, where the average contribution amount for covered workers at small firms ($7,947) is higher than the amount at large firms ($5,697). Eight percent of covered workers, including 21% of covered workers at small firms, are in a plan with a worker contribution of $12,000 or more for family coverage.
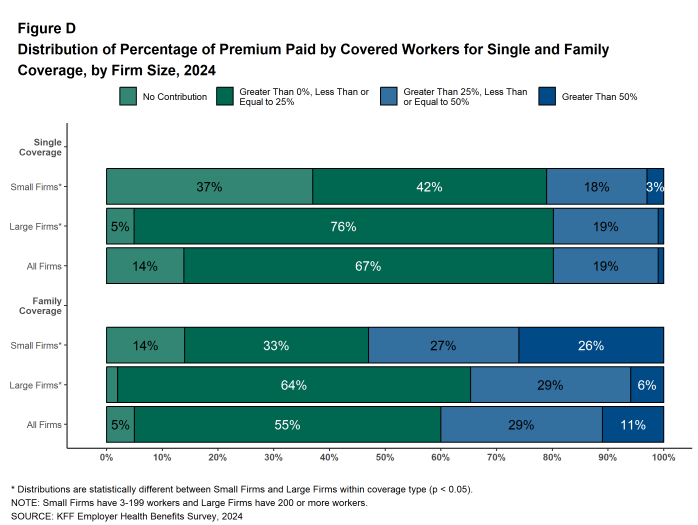
Figure D: Distribution of Percentage of Premium Paid by Covered Workers for Single and Family Coverage, by Firm Size, 2024
PLAN ENROLLMENT
PPOs remain the most common plan type. In 2024, 48% of covered workers are enrolled in a PPO, 27% in a high-deductible plan with a savings option (HDHP/SO), 13% in an HMO, 11% in a POS plan, and 1% in a conventional (also known as an indemnity) plan [Figure E]. This distribution of covered workers across plan types is similar to the distributions of covered workers by plan type in recent years.
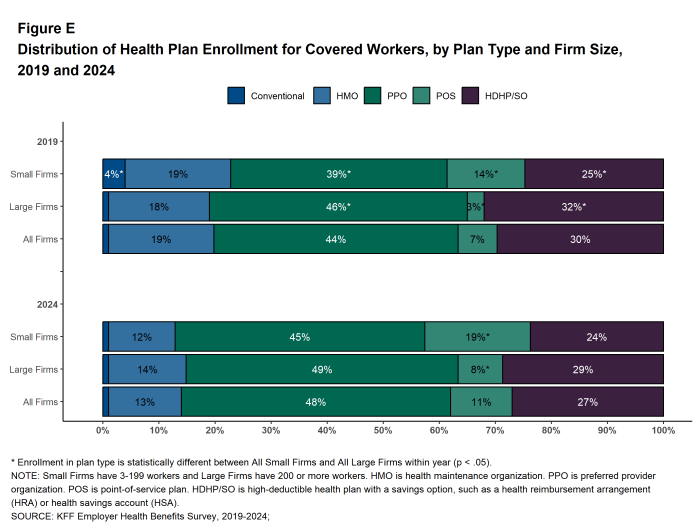
Figure E: Distribution of Health Plan Enrollment for Covered Workers, by Plan Type and Firm Size, 2019 and 2024
SELF FUNDING
Many firms – particularly larger firms – have self-funded health plans, which means that they pay for the health services for their workers directly from their own funds rather than through the purchase of health insurance. Sixty-three percent of covered workers, including 20% of covered workers at small firms and 79% at large firms are enrolled in plans that are self-funded. The percentage of covered workers in self-funded plans in 2024 is similar to last year.
Thirty-six percent of covered workers in small firms offering health benefits are covered by a level-funded plan, similar to the percentage in 2023. Level-funded arrangements combine a relatively small self-funded component with stop-loss insurance, which limits the employer’s liability and transfers a substantial share of the risk to insurers. These plans have the potential to meaningfully affect competition in the small group market because, unlike insured plans, they use health status as a factor in rating and underwriting and are not required to provide all of the essential health benefits that are mandatory for other plans.
.
EMPLOYEE COST SHARING
Eighty-seven percent of workers with single coverage have a general annual deductible that must be met before most services are paid for by the plan, similar to the percentage last year (90%).
The average deductible amount in 2024 for workers with single coverage and a general annual deductible is $1,787, similar to last year. The average deductible is higher for covered workers at small firms ($2,575) than at large firms ($1,538). Among workers with single coverage and an annual deductible, the average amount is similar to the deductible amount five years ago ($1,655) but is 47% higher than the amount ten years ago.
In 2024, 32% of covered workers are in a plan with a general annual deductible of $2,000 or more for single coverage, similar to the percentage (31%) last year. Covered workers in small firms are more likely than those in large firms to be in such a plan (50% vs. 26%). The percentage of covered workers with a general annual deductible of $2,000 or more for single coverage has grown over the last ten years, from 18% to 32% [Figure F].
Some workers in health plans with high deductibles also receive contributions to savings accounts from their employers. These contributions can be used to reduce cost sharing amounts. Twenty-five percent of covered workers in an HDHP with a Health Reimbursement Arrangement (HRA), and 2% of covered workers in a Health Savings Account (HSA)-qualified HDHP receive an account contribution for single coverage that is greater than or equal to their deductible amount. Additionally, 24% of covered workers in an HDHP with an HRA and 9% of covered workers in an HSA-qualified HDHP receive account contributions that, if applied to their deductible, would reduce their personal annual liability to less than $1,000.
In addition to any general annual deductible they may have, most covered workers also pay a portion of the cost of care when they use health care services, typically a copayment (a fixed dollar amount) or coinsurance (a percentage of the covered amount). For physician office visits, the average copayments are $26 for a primary care visit and $42 for a visit to a specialist. The average coinsurance rate is 20% for both primary care and specialist visits. All of these amounts are similar to the amounts in 2023.
When admitted to the hospital, 59% of covered workers have coinsurance requirements, 16% have a copayment, and 9% have both a copayment and coinsurance requirement. The average coinsurance rate for a hospital admission is 21% and the average copayment amount is $343. The cost sharing requirements for outpatient surgery follow a similar pattern to those for hospital admissions, although the average copayment amount for outpatient surgery is lower, at $216.
Virtually all covered workers are in plans with an annual limit on in-network cost sharing (called an out-of-pocket maximum) for single coverage, though these limits vary significantly. Among covered workers in plans with an out-of-pocket maximum for single coverage, 14% are in a plan with an out-of-pocket limit of $2,000 or less, while 24% are in a plan with a limit above $6,000.
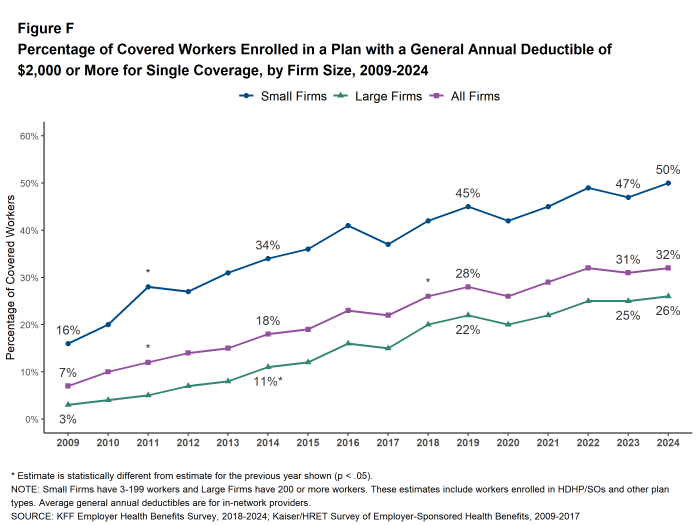
Figure F: Percentage of Covered Workers Enrolled in a Plan With a General Annual Deductible of $2,000 or More for Single Coverage, by Firm Size, 2009-2024
AVAILABILITY OF COVERAGE FOR SPOUSES OF COVERED WORKERS
A very large share of firms that offer health benefits offer to cover dependents of covered workers. Among firms offering health benefits, 95 percent of firms with 10 to 49 employees and virtually all (99%) larger firms offered spouses an opportunity to enroll.
Among firms with 200 or more workers offering coverage to spouses, 10% do not allow the spouse to enroll if they are offered health insurance from another source, 13% place conditions on spouses wishing to enroll, such as limiting plan choice, or requiring a surcharge for enrolling spouses if they are offered coverage from another source. Among firms with 200 or more workers offering coverage to spouses, 8% require a surcharge for spouses who are offered coverage from another source.
.
GLP-1 DRUG COVERAGE FOR WEIGHT LOSS
GLP-1 (Glucagon-like peptide-1) agonists, used to help control blood sugar levels in people with type 2 diabetes, have also been shown to be an effective drug to help people lose weight. However, the high cost of these drugs, combined with the large number of people who could benefit and the potential for long-term usage, has raised questions about the potential costs to plans that cover them.
Eighteen percent of firms with 200 or more employees, including 25% of firms with 1,000 or more employees, cover GLP-1 agonists when used primarily for weight loss. Firms with 200 to 999 employees are more likely than larger firms to respond that they do not to know to this question [Figure G].
Among firms with 200 or more employees that provide coverage for GLP-1 agonists primarily for weight loss, 53% have some type of condition or requirement associated with covering these medications. These include 24% that require employees to meet with a professional, such as a dietitian, psychologist, case worker, or therapist before approving a GLP-1 drug prescription, 8% that require employees to enroll in a lifestyle or weight loss program for a period of time before approving a GLP-1 drug prescription and 10% that require employees to enroll in lifestyle or weight loss program while taking GLP-1 drugs.
Firms with 200 or more employees covering GLP-1 agonists primarily for weight loss were asked about the potential impacts on costs and employee satisfaction. Thirty-three percent of these firms, including 58% of firms with 5,000 or more employees, say that covering these medications for weight loss will have a “significant impact” on their prescription drug spending. Sixteen percent of firms offering health benefits say that covering these medications for weight loss will be “very important” for employees’ satisfaction with their health plan, including 28% which currently cover GLP-1 agonists for weight loss [Figure H].
Among firms with 200 or more employees that do not provide coverage for GLP-1 agonists primarily for weight loss, 62% say that they are “not likely” to begin covering these medications for weight loss within the next twelve months, 23% say that they are “somewhat likely” to do so, 3% say that they are “very likely” to do so, and 11% do not know.
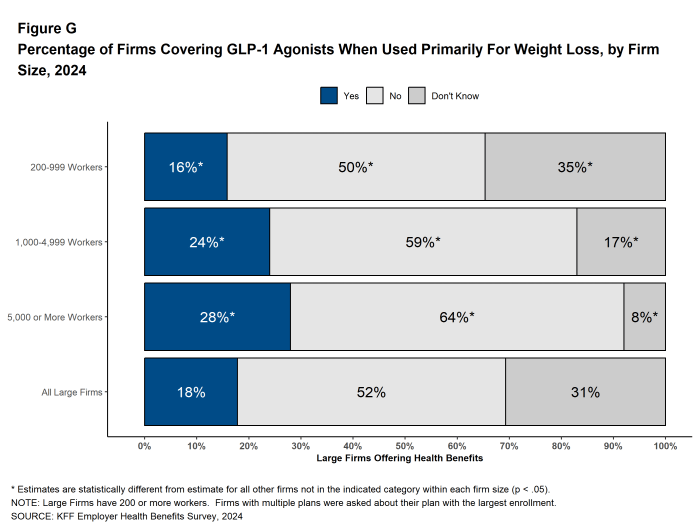
Figure G: Percentage of Firms Covering Glp-1 Agonists When Used Primarily for Weight Loss, by Firm Size, 2024
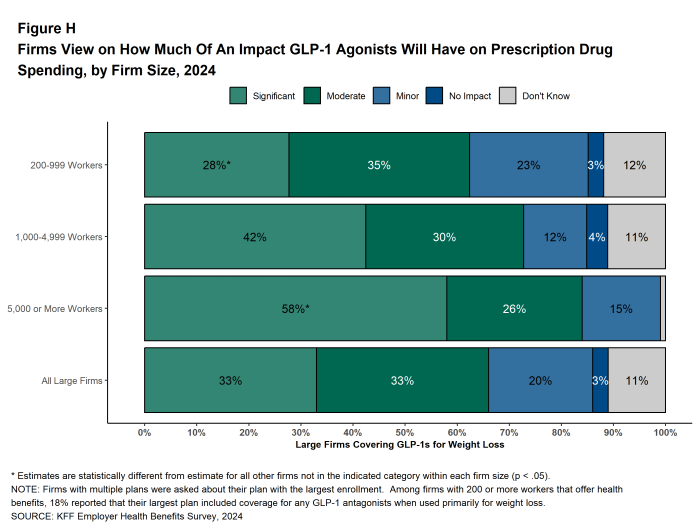
Figure H: Firms View On How Much of an Impact Glp-1 Agonists Will Have On Prescription Drug Spending, by Firm Size, 2024
HEALTH PLAN PROVIDER NETWORKS
Tiered and Narrow Networks. Health plans structure their networks of providers to provide access to care and to encourage enrollees to use providers that are lower cost, or that provide better care. One option to accomplish these goals are high-performance or tiered network plans, which use cost-sharing or other incentives to encourage enrollees to use in-network providers that have better performance or quality, or have lower costs. Another option are narrow network plans, which significantly restrict the number of participating providers in order to reduce costs.
Among firms with 50 or more employees that offer health benefits, 20% have a high-performance network or tiered network as part of their health plan with the largest enrollment in 2024. Firms with 1,000 or more employees are more likely to include a high-performance or tiered network in their largest health plan than smaller employers (27% vs. 20%). Eight percent of firms with 50 or more employees that offer health benefits offer a health plan that can be considered a narrow network in 2024, similar to the percentage last year (11%). Firms with 5,000 or more employees are more likely to offer a narrow network plan than employers with fewer employees (18% vs. 8%).
Employer Views on the Breadth of Their Provider Networks.
Employers that offer health benefits were asked to characterize the breadth of the provider network in their plan with the largest enrollment overall, and for services for mental health and substance use conditions.
Fifty-four percent of firms characterize the network in their plan with the largest enrollment as ‘very broad,’ 35% say it is ‘somewhat broad’, and 10% say it is ‘somewhat narrow’ or ‘very narrow’. Firms with 200 or more employees are more likely than smaller firms to characterize the provider network in their plan with the largest enrollment as “very broad” (68% vs. 54%).
Thirty percent of firms characterize the network in their plan with the largest enrollment as ‘very broad’ for mental health and substance use condition services, 45% say it is ‘somewhat broad’ for these services, and 24% say it is ‘somewhat narrow’ or ‘very narrow’. Firms with 200 or more employees are more likely than smaller firms to characterize the provider network in their plan with the largest enrollment as “very broad” for mental health and substance use condition services (46% vs. 30%) [Figure I].
Employers that offer health benefits are less likely to characterize their network with the largest enrollment as ‘very broad’ for mental health and substance use condition services than for medical services overall. This is true for small firms (3 to 199 employees) (30% vs. 54%) and larger firms (46% vs. 68%). However, 48% of large employers have increased the number of mental health counseling resources available to employees through an employee assistance program or some other third-party vendors, such as Headspace or Lyra Health.
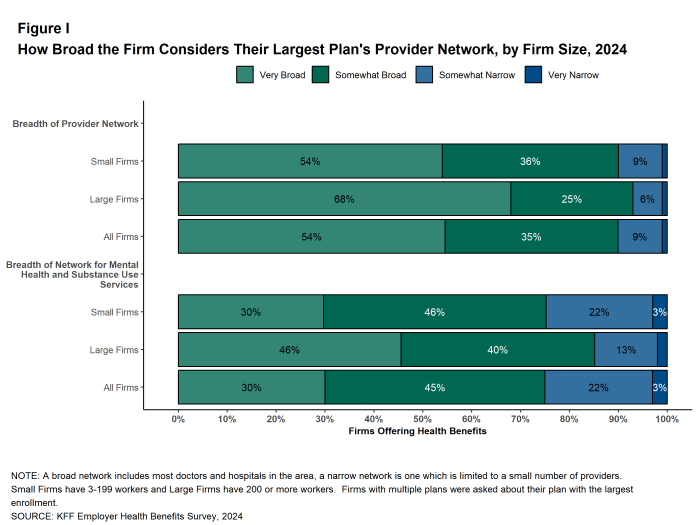
Figure I: How Broad the Firm Considers Their Largest Plan’s Provider Network, by Firm Size, 2024
BENEFITS FOR FAMILY BUILDING SERVICES
Some employers have introduced benefits to help employees trying to conceive or adopt a child. Among firms with 200 or more employees that offer health benefits, 37% provide coverage for fertility medications in their plan with the largest enrollment, 26% provide coverage for intrauterine (artificial) insemination, 27% provide coverage for in-vitro fertilization (IVF), 12% provide coverage for cryopreservation, sometimes called egg or sperm freezing, 13% provide coverage for adoption services, and 7% have coverage for other family-building services. Many large employers were uncertain about their coverage of family building benefits and reported don’t know, including 29% for fertility medications, 32% for artificial insemination, 30% for IVF, 38% for cryopreservation and 26% for adoption.
.
PRICE AND COST SHARING INFORMATION FOR ENROLLEES
New federal rules require health plans (including self-funded plans) to make information available to enrollees about the estimated cost of services and cost-sharing on a “real-time” basis. Among firms with 200 or more employees that offer health benefits, 41% say that providing employees with additional information about the cost of services will help their health care decision making “a great deal”, 38% of these firms say that it will help their decision making “somewhat”, 15% say that it will help their decision making “very little”, and 2% say that it will help their decision making “not at all”. Thirteen percent of these firms say that the new requirements will reduce health spending “a great deal”, 50% say that the new requirements will reduce health spending “somewhat”, 24% say that the new requirements will reduce health spending “very little”, and 7% say that the new requirements will reduce health spending “not at all”.
.
ABORTION SERVICES
The United States Supreme Court decision in Dobbs vs. Jackson, and subsequent state activity to regulate abortion has increased interest in coverage for abortion services in employer plans. Firms with 200 or more employees offering health benefits were asked which of several statements best described the coverage of abortion services in their largest health plan.
- Twenty-nine percent of these firms said that legally provided abortions are covered in most or all circumstances (sometimes referred to as elective or voluntary abortion). Firms with 5,000 or more workers were more likely than smaller firms to give this response (39%) [Figure J].
- Eighteen percent of these firms said that legally provided abortions are covered only under limited circumstances, such as rape, incest, or health or life endangerment of the pregnant enrollee. Firms with 5,000 or more workers were more likely than smaller firms to give this reply (31%).
- Eight percent of these firms said that legally provided abortions are not covered under any circumstance. Firms reporting that legally provided abortions are not covered were asked to confirm that their largest plan would not cover abortion under any circumstance, even in states where abortion was legal. In total, 81% verified this was their policy.
- Forty-five percent of responding firms answered “Don’t know” to this question. Respondents with 200 to 999 workers were more likely than other respondents to answer, “Don’t know,” while respondents with 1,000 to 4,999 workers and 5,000 or more workers were less likely to do so.
Five percent of large firms offering health benefits currently provide or plan to provide financial assistance for travel expenses for enrollees who travel out of state to obtain an abortion if they do not have access near their home. Firms with 5,000 or more workers are more likely than other firms to say they provide or plan to provide travel benefits (21% vs. 5%).
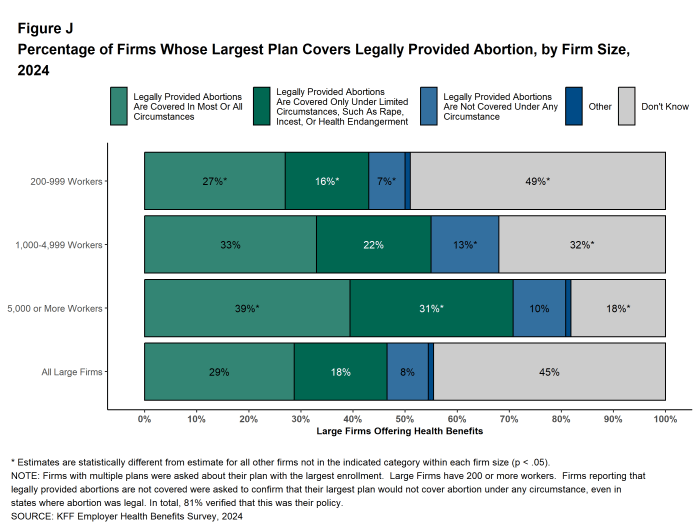
Figure J: Percentage of Firms Whose Largest Plan Covers Legally Provided Abortion, by Firm Size, 2024
ASSISTANCE FOR LOWER-WAGE WORKERS
Some firms have programs to make it easier for lower-wage workers to afford to enroll in a health plan. Among firms with 200 or more employees offering health benefits, 6% have a program that reduces cost sharing for lower-wage workers and 14% have a program that reduces their premium contributions.
Employers with 5,000 or more workers are relatively more likely to have a program that reduces premium contributions for lower-wage workers while employers with 200 to 999 employees are relatively less likely to have such a program. Fourteen percent of these firms offer a plan with reduced benefits and a low premium contribution to make it affordable for lower-wage workers.
.
DISCUSSION
The average annual premium increased 6% for single coverage and 7% for family coverage in 2024, similar to the rates in 2023. These increases likely reflect higher prices for health care, which have followed the higher prices in the rest of the economy over the last several years. Changes in premiums can lag other economic measures because insurers lock in prospective prices with providers. Therefore, it may take some time for premium changes to reflect the more modest inflation in 2024. Looking over a longer period, family premiums have grown 24% over the last five years, roughly comparable to the rate of inflation (23%) and the change in wages (28%) over the period.
Unlike the change in premiums, deductible amounts have been stable for several years, though they are still quite high. The average deductible in 2024 for single coverage among those with a deductible ($1,787) is not statistically different than last year ($1,735) nor five years ago ($1,655).
Whether and how to cover GLP-1 agonists when used primarily for weight loss has been a much-discussed issue for employers and other public and private health insurance payers. These drugs, which have recently been shown to be an effective drug to help people lose weight, are quite costly and have the potential to be used for long periods of time. Among employers with 1,000 or more employees, only one-in-four employers cover these drugs when used primarily for weight loss in 2024; 69% of these employers that do not cover them for this purpose say that they are not likely to do so within the next twelve months. Among the one-in-four that do cover them, 46% say that covering these medications for weight loss will have a “significant impact” on their prescription drug spending, while only 31% say that covering these medications for weight loss will be “very important” for employees’ satisfaction with their health plan.
Coverage for these drugs is likely to remain a hot future topic as employers and other payers gain insights about the long-term effectiveness and costs associated with these drugs. A key issue for payers and users of these medications is whether those who use them can eventually maintain lower weights without continued reliance on these medications. Many payers that currently cover these drugs for weight loss have accompanying requirements such as counseling or enrollment in lifestyle or weight loss programs with the hope that users can reduce or eliminate their need for these medications over time. The effectiveness of these programs is likely to be an important factor for employers in their future decision making about whether and how to cover these medications.
.
METHODOLOGY
The KFF 2024 Employer Health Benefits Survey reports findings from a survey of 2,142 randomly selected non-federal public and private employers with three or more workers. Davis Research, LLC conducted the field work between January and July 2024. The overall response rate is 14%, which includes firms that offer and do not offer health benefits. Unless otherwise noted, differences referred to in the text and figures use the 0.05 confidence level as the threshold for significance. Small firms have 3-199 workers unless otherwise noted. Values below 3% are not shown on graphs to improve readability. Some distributions may not sum due to rounding. For more information about survey methodology, see the Survey Design and Methods section at ehbs.kff.org.
Filling the need for trusted information on national health issues, KFF is a nonprofit organization based in San Francisco, California.
link
