

Thirty-one EEs were contacted, of which 15 accepted to participate. Reasons for not participating included distance and limited transportation to the local area where the focus groups meetings took place (n = 10), lack of time / lack of interest (n = 2) and current symptoms of depression or anxiety with clinical significance (n = 3). Sixteen HPs were contacted of which 14 accepted to participate; two withdrew their participation due to limited availability (Table 1).
Major changes produced across templates’ refinement, concerns the elimination of the third order codes by integrating them in second order (see Fig. 1 for an example). The final EEs template included the following second-order codes or themes: (1) Individual impressions about the treatment (including the affective attitude and practicality of the tDCS device, the CBT-based App and their combination); (2) Factors influencing the choice of treatment by EEs; (3) EEs’ preferences for receiving information about the treatment; and (4) Suggestions for improvement. The final HPs template included the following higher-order themes: (1) individual impressions about the treatment (including the affective attitude and practicality of the tDCS device, the CBT-based App and their combination); (2) Factors influencing patients’ choice of the treatment; (3) When, where and from whom should women receive information about the treatment; (4) Factors contributing to the prescription of the treatment; and (5) Suggestions for improvement. For a glance to versions 1 and 5 of the templates including first, second and third order codes, pre- and post-analysis, see Supplemental Files.

Example of hierarchical changes between codes across EEs template refinement where the third order codes were integrated in the second order codes. The example includes only one first order code – Individual impressions about the combined treatment. Blue: Initial version of the template; Green: Final version of the template.
Frequencies of codes were extracted from participants’ narratives, supporting the identification of patterns across cases. Frequencies correspond to the number of meaning units per second-order code (e.g. “2/4” correspond to 2 entries of one meaning unit out of the total entries among all meaning units within one second-order code). For the full list of first-order codes, second-order codes and meaning units, see Figure S1 on Supplemental Files.
Experts by experience (EEs)
Individual impressions about the treatment
EEs affective attitude about the treatment were mainly positive (74%). The combination of tDCS with an app captured EEs interest in its innovative nature (2/4) and enthusiasm (1/4) and, to a lesser degree, apprehension (1/4). EEs were mostly enthusiastic about the device (6/8) but feared its safety and potential misuse (2/8).
Yes, just the fact that it is non-invasive is super interesting (P1G5).
The affective attitude towards the app was mostly positive (73%) with EEs being pleased (4/11) and drawn to the app (3/11). However, there were also feelings of disappointment with the lack of human interaction (1/11) and embarrassment with the language (1/11).
Some questions that make us feel embarrassed or less comfortable (P1G3).
In terms of practicality, the combined treatment was perceived positively (92%), considering the advantages offered for clinical monitoring and treatment compliance (2/12), its usefulness and suitability (3/12), simplicity (1/12), convenience of a home-based treatment (2/12) and safety (2/12). However, EEs were apprehensive about the limits of exclusively bot-lead interventions (1/12). The connection of the device with the clinician’s platform for monitoring was appreciated (2/7), considered convenient (1/7) and the device considered simple to use (1/7). However, EEs also mentioned the device apparent fragility (1/7), shared their apprehension when using it (1/7) and fears of being autonomous in administering tDCS (1/7) by themselves.
The experience with the app was generally positive (57%) with the app being experienced as advantageous for self-monitoring of symptoms (1/46), simple (3/46), convenient (2/46), highly customizable (7/46), user-friendly (2/46), discreet (2/46), flexible (4/46), suitable (1/46), informative (2/46), and useful (2/46). For some the language was not suitable (7/47). Simultaneously, the app’s inability to replace face-to-face interactions (8/47), the limits on its customization (1/47), the time of CBT sessions (30 min; 3/47) and the expected progressive loss of adhesion by users (1/47) were issues raised.
I believe that those dealing with anxiety and emotions need someone, face-to-face (P1G3).
Factors influencing the choice of treatment
For EEs, the safety profile, namely short- and long-term adverse effects of the treatment, both on the fetus and the mother, during pregnancy and breastfeeding, was the factor to start treatment with the highest weight (22%).
We think that we will harm them, that something will pass into the milk, but it actually doesn’t have that side effect, so it ends up being better (P2G4).
EEs’ perception about treatment efficacy depended on having access to reliable information about the treatment (18%) from HPs (7/14), scientific literature (6/14), or real-life testimonials (1/14), increasing the likelihood of choosing the treatment, and building trust and confidence in the intervention. The alignment with individual values weighted 17.5% on the decision to uptake the treatment, namely as a medication-free (6/13) alternative, the freedom to choose treatments according to individual preferences (2/13), novelty and curiosity (2/13), differentiation (1/13), non-invasiveness (1/13) and the non-stigmatizing nature of the treatment (1/13).
Because it’s something different and not medication based, I would choose that (P1G1).
Costs and efforts associated with the treatment weighted 22% on the decision to uptake the treatment. The home-based nature was aligned with women’s needs (4/9), extending accessibility to treatments (3/9).
(…) also the fact that we can control the time we dedicate to the process is a good thing, and it helps avoid travel (P3G3).
The low monetary cost was additionally considered (2/9). In terms of efforts, the convenience of a home-based treatment (4/9) and the potential shorter time to response to treatment (4/9) contributed to the treatment uptake. However, the higher monetary value of this treatment compared to medication (due to lack of coverage by insurances) (1/9) and the increased time required to complete one session vs. taking a daily pill (2/9) were of concern. As of contextual factors, the presence of symptoms impacting daily functioning weighted 8% when choosing this treatment.
EEs acknowledge that each case is unique (2/7), that the treatment could be particularly interesting to technologically savvy (4/7) and younger women (1/7) with some health literacy (1/7).
Preferences about receiving information about the treatment
Most EEs prefer to receive information from a mental healthcare professional (unspecified (2/23), psychiatrist or psychologist; 6/23), obstetrician (5/23), general practitioner (4/23), nurse (1/23) or HP from the maternity (1/23)) or a tDCS expert (4/23). Information should be delivered before pregnancy (2/30), during pregnancy (11/30), before symptoms onset (6/30), at early stages of disease (5/30), at any time (4/30), or depending on the woman’s individual situation (2/30).
After childbirth, a woman is 100% focused on the baby. Her attention is largely directed towards the baby, which is why, in my opinion, it’s important to provide information beforehand rather than afterward (P1G1).
Suggestions for improvement
A total of 61 entries were suggestions, most of them about the app. These included content topics (6/61) such as customization to the perinatal population (3/6) and personalization to individual needs (3/6). Suggestions concerning the structure (5/61) included the reduction of the initial questioning (3/5), and gamification (1/5). Suggestions for enhanced functionality included having all content available in the app in the mother tongue of the user (2/16), integration of headphones (1/16), face-to-face or online interactions with health professionals (9/16), enabling appointment on-demand (1/16), integration of physical and mental health care (1/16), a forum or community (1/16), and the mandatory usage of the app when switching-on the tDCS device (1/16). Additionally, a broad reaching communication strategy/campaign about the availability of this treatment would be welcome (1/61).
It would be amazing if it were possible to use headphones and microphones with the helmet and if the sessions were synchronous, with the stimulation session happening simultaneously with the app session, providing guided sessions on nutrition and relaxation music and similar things (P3G2).
Health professionals
Individual impressions about the treatment
HPs affective attitude towards the combined treatment was mixed (33% positive and 67% negative), with one enthusiastic reference to the advantages of self-administered treatments (1/5), but several others expressing concerns about the limitations of exclusively remote/virtual and bot-lead interventions (4/5).
HPs affective attitudes toward the tDCS device were also mixed, with some appreciating its comfort and appearance (1/3) and the availability of an alternative treatment (1/3), alongside fear (1/3). Most HPs identified positive practical aspects of the device (10/13), such as the convenience of its home-based nature in the context of the limited resources in the public health system (1/13) and the flexibility to be completed at the same time as other activities (2/13). The experienced comfort of the headset (3/13), its resistance (1/13), simplicity (1/13), and safety profile (2/13) were positively weighted. On the other hand, HPs showed apprehensiveness concerning the size of the headset (male HP; 2/13) and the lack of human interactions (1/13).
(…) it makes things much easier because it allows them [women] to make better use of their time (P4G2).
HPs’ affective attitude towards the app was mostly positive (69%) with many being drawn to it (4/13), pleased (4/13) and enthusiastic (1/13), referring to how it fostered interactions that felt close to natural, and within an aesthetically pleasing and user-friendly interface. However, for some the style was too condescending (2/13). Additionally, there was some apprehension about the limitations of bot-lead interventions (2/13).
HP’s feedback about the app’s practicability included positive (41%) and negative (59%) references. The autonomy promoted by the app, its simple and flexible use, and the clinician’s dashboard for clinical monitoring were considered convenient (5/13). The topics embedded in the CBT sessions were considered of relevance (5/13), useful (1/13), adjusted (1/13) and its accessibility convenient (1/13). In fact, as a stand-alone intervention, the app was seen as a viable alternative to traditional methods, offering a comprehensive solution (more than the stand-alone tDCS), and a complementary intervention for primary care in PPD, representing by itself a significant advancement in mental health care.
In terms of application, I think it benefits from the fact that you can do it at home, whenever you want, however you want (…)(P3G3).
As for negative aspects related to the app, HPs identified algorithm constraints that limit personalization (1/19), potential language barriers (despite the subtitles in psychoeducational videos; 2/19), limited clinical monitorization (3/19), limits to exclusively bot-lead psychological interventions (2/19), the overall absence of human interaction (3/19), and concerns about feelings of loneliness by already depressed patients (1/19). The commonly high dropout rates for digital health interventions (2/19) and concerns about patient’s data protection (5/19) were also raised.
(…) the visual expression, the contact allows us doctors to draw several conclusions about the course of treatment… (P3G2).
Factors influencing women’s choice of the treatment
HPs discussed six factors contributing to women’s choice of treatment. Costs represented 29% of the intercessions, safety 27%, needs/values 20%, perception of treatment efficacy 13%, contextual factors 9% and confidence to self-administer the treatment 2%. HPs considered that communication should be offered by HPs (2/7) and disseminated by influencers/testimonials (1/7) and it strongly influences women’s perception of treatment efficacy and safety, and consequently their choice (7/7).
It has to be introduced by a professional (…) this gives credibility, gives a sense of security… (P3G2).
Women’s perception about its safety profile and side effects for the fetus/newborn (6/15) or both the fetus and mothers (9/15) is highly valued, addressing the concerns of those women reluctant to medication.
If there is this possibility, and it is non-pharmacological, if it is a way of overcoming it without medication, perhaps it is much more acceptable (P3G3).
Contextual factors influencing the adoption of the treatment by women included family support (3/5), women’s insight about their clinical condition (1/5) and acceptance of their condition (1/5). In terms of costs, HPs considered that women would value treatment’s accessibility (9/16), low monetary cost (2/16), and the potential short time to respond to treatment (1/16).
(…) many people miss appointments, even at the hospital level, because they are unable to go to the hospital (P2G3).
However, the high levels of commitment required for self-delivered treatments (2/16; when compared to traditional medication), could lead to dropouts, supporting the need to implement strategies to ensure consistent treatment schedules at home. For some women the home-based nature with reduced human interactions (2/16) were pointed as extra effort decreasing the chances of choosing this treatment. In that sense, this treatment might be in contrast with some women’s needs of human interaction (2/11). On the other hand, managing therapy privately was seen in line with women’s fears of stigma (4/11) and their need to feel free to choose (3/11), contributing to the treatment uptake. Similarly, while those women reluctant to medication would most probably accept the treatment (1/11), misconceptions about non-invasive brain stimulation treatments can affect acceptance (1/11).
When, where and from whom should women receive information about the treatment
According to HPs, women should be informed about PPD treatments before being pregnant / during pregnancy (6/10), or after childbirth (4/10), and treatment options should be discussed after symptoms’ onset (10/14), although before symptoms onset was also considered acceptable as a preventive action (4/14). Information should be delivered at the primary (2/5) or secondary (2/5) care services, or both (1/5), by any health care professional (3/16) including nurses (1/16), psychologists (1/16), medical doctor (1/16), GPs (2/16), obstetricians (2/16), psychiatrists (1/16) or any professional as long as they are integrated in a maternal health team and are properly trained (5/16).
Factors contributing to the prescription of the treatment
HPs discussed seven factors contributing to treatment prescription, including the patient’s profile (weighting 56%), values (13.5%), costs (11%), self-confidence to support self-administration of treatment by patients (9.5%), perception of efficacy (4%), efforts (3%), and safety (1.5%). Hence a new third order code arose concerning clinician’s reasoning (1.5%).
Women to whom the treatment would be most beneficial include those reluctant to medication (7/44) or presenting adverse effects to medication (1/44) and those motivated to complete this type of treatment autonomously (4/44), preferring home-based or remote options (4/44), or with low adhesion to other treatments (1/44). The treatment should be prescribed to pregnant (1/44) or breastfeeding (2/44) women, presenting mild to moderate symptoms of anxiety or depression (7/44), and/or risk factors to develop PPD (such as previous mental health conditions; 4/44).
It depends. For example, we have milder symptoms that can be treated with psychotherapy or some other type of treatment, or even as part of a strategy for augmenting antidepressants (P3G1).
Typically, younger women (1/44) with higher educational degree (3/44) and good technological literacy (2/44) would benefit more than women with low education (3/44) or women in need of increased contact with health professionals (3/44). The patient’s personality was also considered (1/44).
The treatment should be considered either as adjunctive treatment when patients present adverse effects to antidepressants, or as first-line option (1/1). HPs showed confidence in educating their patients on the behaviors required for a successful treatment (7/7). Perception of treatment efficacy was consensual (3/3). The information available to HPs about the safety of the treatment (either from scientific literature sources [1/3] or out of experience [1/3]) were identified as factors driving prescription.
The opportunity of extending treatment options (2/9) and broadening accessibility to health care (3/9) were encouraging factors whereas ethical dilemmas about non-human-led interventions, AI-based diagnosis (3/9) and potential undesirable results from indirect monitoring of remotely supervised treatments (1/9) were discouraging. To a smaller degree, the efforts required to deal with stigma around brain stimulation (1/2) and the time required to educate patients (1/2) were considered.
(…) if the postpartum woman undergoes this treatment at home, managing it herself for a total of six weeks, there is no guarantee that she won’t be worse by the end of the process. Meanwhile, valuable time has been lost (P2G3).
Finally, HPs’ values concerning patient’s autonomy (4/10), patient’s freedom of choice (5/10) and the ambition for a universal perinatal mental health care program (given the limited capacity of the public health systems [1/10]) were added as driving prescription.
… if there is a clinical indication, be transparent and give the patient the choice…” (P4G1).
Suggestions for improvement
Several suggestions were offered by HPs, mainly app related. An increased focus of the app content on specific topics related to maternal/perinatal mental health is needed, including clinical and emotional aspects of pregnancy, attachment, postpartum, newborn care, and the negative impact of depression on the fetus/newborn (19/81). Customization features according to distinctive clusters of PPD symptoms, the perinatal period or individual preferences were brought up (12/81). Language adjustments were suggested (4/81) but the degree of formality/directiveness varied according to individual preferences. Structural changes to the app were suggested, including reducing the introductory parts achievable by transferring the introduction to the treatment to an in-person consultation (4/81). Most importantly, HPs agreed on the need to complement self-administered tDCS, self-lead digital intervention and remote monitoring with face-to-face sessions with an HP (32/81). For a synthesis see Table 2; Fig. 2.
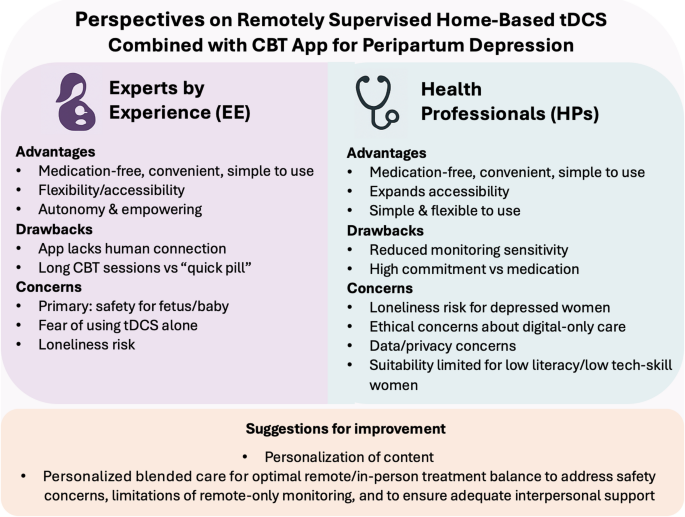
Major takeaways from EEs and HPs evaluations: Advantages, drawbacks and concerns about the FLOW solution.
link
